Targeting Inflammation
Assessing both obesity and inflammation together is important because they are closely connected and can lead to serious health problems if ignored. Doctors often use tools like BMI, waist circumference, and blood tests to look for markers of inflammation to get a fuller picture of the health of the person they are treating. By measuring both weight-related factors and inflammatory signals, healthcare providers can identify risks earlier, such as the chance of developing diabetes or heart disease. This kind of assessment helps create a more complete understanding of how excess fat is affecting the body beyond just weight gain.1,2
Treatment strategies that target both obesity and inflammation may be more effective than focusing on one alone. Lifestyle changes like healthy eating, regular exercise, and stress management can reduce body fat and lower inflammation at the same time. In some cases, medications or surgery may be recommended, but these are usually combined with long-term behavior changes to keep inflammation under control. By addressing both conditions together, patients can improve their overall health, lower their risk of chronic diseases, and build a stronger foundation for long-term wellness.1,2,3
Strategies that target inflammation—either directly or through weight reduction—can significantly improve clinical outcomes.4 Improving lifestyle habits, in terms of nutrition (e.g., energy-reduced diet, adjusted macronutrient ratio, etc.) and frequency/type of physical activity, remains a cornerstone of obesity management.5
Medications
Anti-obesity medications have served an increasingly important role in obesity treatment and should be administered together with lifestyle interventions. Early agents include orlistat, which modifies digestive tract absorption, and centrally acting drugs, such as phentermine-topiramate and naltrexone-bupropion, which regulate appetite in the brain.6

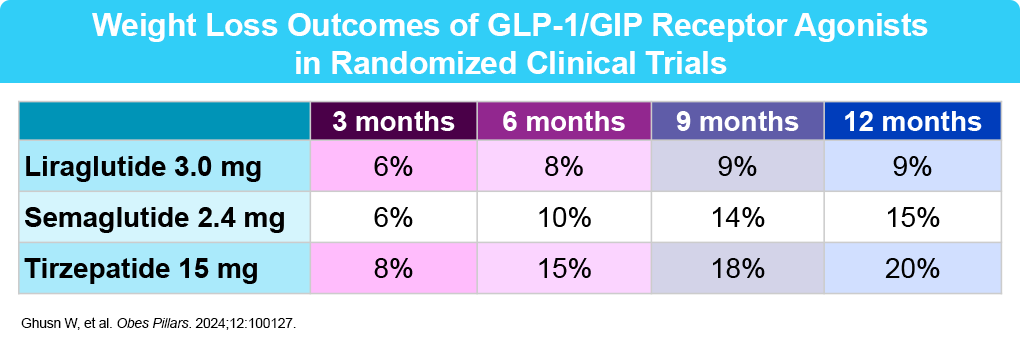
Recently approved anti-obesity medications include glucagon-like peptide-1 (GLP-1) receptor agonists (liraglutide and semaglutide) and a combined GLP-1 and glucose-dependent insulinotropic polypeptide (GIP) agonist (tirzepatide).7 Overall, these medications work by slowing digestion, reducing appetite, and decreasing cravings. Some, like liraglutide, require daily injections, while the others (semaglutide and tirzepatide) are typically administered weekly.8,9 At this time, there are two GLP-1 daily pill formulations approved by the FDA for weight loss. Oral semaglutide was approved in December 2025. Orforglipron, a small-molecule, nonpeptide oral GLP-1 RA with similarly strong weight loss results in clinical trials, was approved by the FDA on April 1, 2026.10 In general, these agents are well tolerated. The side effect profile includes mostly mild to moderate GI side effects (nausea, diarrhea, constipation, vomiting).
Other interventions for treating obesity include endoscopic and bariatric procedures, and psychotherapy, each of which has a role in overall obesity/inflammation treatment.
References
- Steelman G, et al. Evaluation and Treatment Essentials. Accessed 1/7/26. https://www.abom.org/wp-content/uploads/2016/06/Obesity-Evaluation-and-Treatment-Essentials.pdf
- Shneyderman M, et al. Gastroenterol Hepatol(NY). 2024;20(12):712-722.
- Kushner RF. Circulation. 2012;126(24):2870-7.
- Wong HJ, et al. Diabetes Care. 2025;48:292-300.
- Gkrinia EMM, Belančić A. Curr Issues Mol Biol. 2025;47:357.
- Gudzune K, et al. JAMA. 2024;332:571-584.
- Ghusn W, et al. Obes Pillars. 2024;12:100127.
- Moore PW, et al. Adv Ther. 2023;40:723-742.
- Obesity Disease Education Resources – Lilly Medical Education. Medical.lilly.com. Accessed 1/7/26. https://medical.lilly.com/us/diseases/disease-education-resources/obesity/obesity
- Wharton S, et al. N Engl J Med. 2025;393:1796-1806.
