Rheumatology Spotlight
Obesity contributes to the onset, severity, and treatment resistance of several rheumatologic conditions through mechanical stress, systemic inflammation, and immune dysregulation. Obesity is a major risk factor for rheumatologic conditions such as osteoarthritis (OA), particularly in weight-bearing joints such as the knees and hips. The mechanical load from excess body weight accelerates cartilage wear, while adipose tissue secretes pro-inflammatory adipokines like leptin and resistin that exacerbate joint inflammation and degradation.1 Beyond mechanical load, obesity also increases the risk of hand OA, suggesting that systemic metabolic effects—not just mechanical stress—play a role.2,3
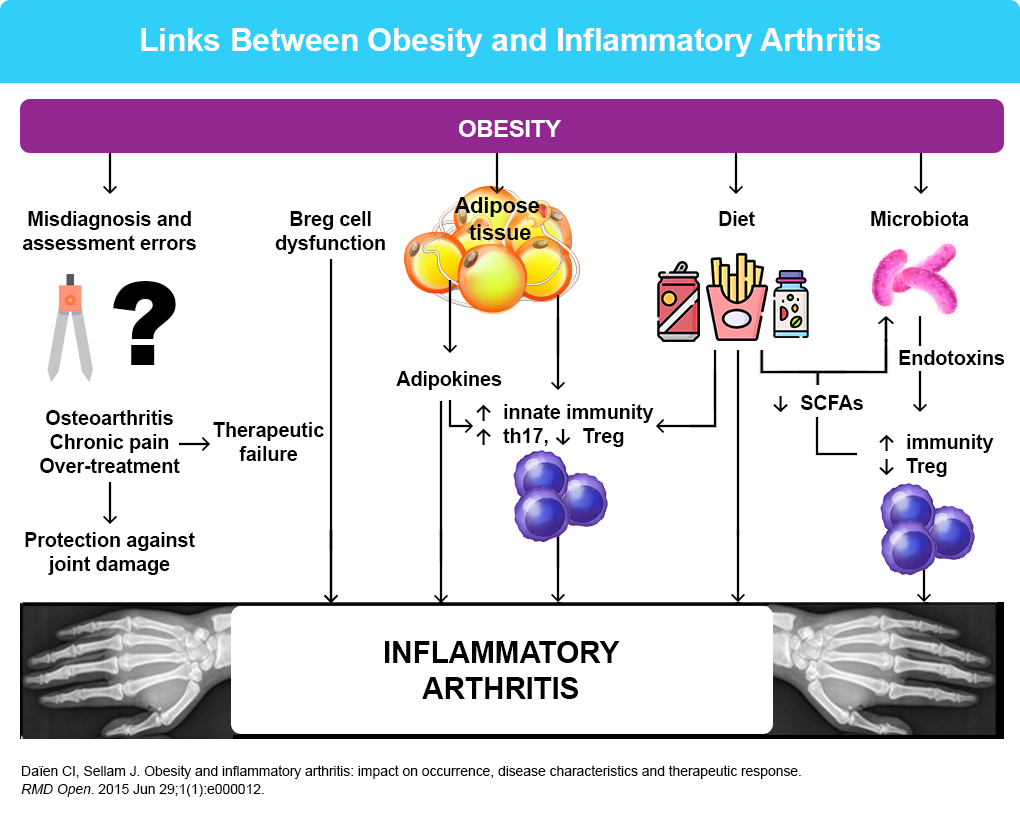
In autoimmune rheumatic diseases, such as psoriatic arthritis (PsA) and rheumatoid arthritis (RA), obesity is associated with higher disease activity and poorer treatment outcomes as well. Patients living with obesity and RA often exhibit reduced responsiveness to TNF inhibitors and lower rates of remission, likely due to chronic low-grade inflammation and altered pharmacokinetics.4 Similarly, obesity in PsA is linked to increased disease severity and a higher prevalence of comorbidities like metabolic syndrome and cardiovascular disease.5 These associations suggest that adiposity may amplify immune dysregulation and interfere with therapeutic efficacy.
Weight loss induced by bariatric surgery has been shown to decrease the risk of PsA and improves disease activity and remission in RA. A 5% weight loss through a low-calorie diet improves the response to TNF inhibitors in PsA; losing even more weight improves the response. In RA, the beneficial effect of weight loss from a low-calorie diet on disease activity has been reported in observational studies.
With regard to weight loss medications, data have shown that individuals treated with GLP‐1 receptor agonists experienced significantly greater reductions in RA disease activity, pain, body weight, total cholesterol, and glycosylated hemoglobin compared with individuals in the control group (P < 0.05). Within the treatment group, there were also significant reductions in erythrocyte sedimentation rate, C‐reactive protein values, LDL-cholesterol values, and triglyceride values.6,7
As a result, weight management is a critical component of rheumatologic care. Studies show that even modest weight loss can improve pain, physical function, and quality of life, and may enhance treatment response in inflammatory arthritic conditions. A multidisciplinary approach—including rheumatologists, dietitians, and physical therapists—is essential to address the complex interplay between obesity and rheumatologic disease and to optimize long-term outcomes.
References
- Conde J, et al. Arthritis. 2011;2011:203901.
- Carman WJ, et al. Am J Epidemiol. 1994;139:119-129.
- Daïen CI, Sellam J. RMD Open. 2015;1:e000012.
- Poudel DR, Karmacharya P. Semin Arthritis Rheum. 2017;47:e2.
- Kumthekar A, Ogdie A. Rheumatol Ther. 2020;7:447-456.
- Tournadre A, Beauger M. Joint Bone Spine. 2024;91:105647.
- Kellner DA, et al. ACR Open Rheumatol. 2025;7:e70103.
