Gastroenterology Spotlight
The incidence of gastrointestinal conditions such as inflammatory bowel disease (IBD) is rising in parallel with the number of individuals who are overweight or obese. Contrary to conventional belief, approximately 15% to 40% of patients with IBD are obese, which might contribute to the development of IBD.1 In a systematic review of 260 population-based studies, the estimated annual incidence of IBD ranged from 10–30 cases per 100,000 persons in the Western world; an estimated 0.5% of adults in the West suffer from IBD.1 The incidence of IBD has increased over time, especially in newly industrialized countries.2,3
The high prevalence of obesity in patients with IBD suggests an independent effect of IBD on the risk of obesity development. Although current epidemiological data are unable to accurately assess the directionality of this association, preclinical data suggest that dysbiosis and altered metabolic gut signaling are induced by IBD. Other molecules including incretins, satiety-related peptides (e.g., ghrelin and peptide YY), and bile acids might contribute to the development of obesity and dysmetabolism in patients with IBD.4,5,6
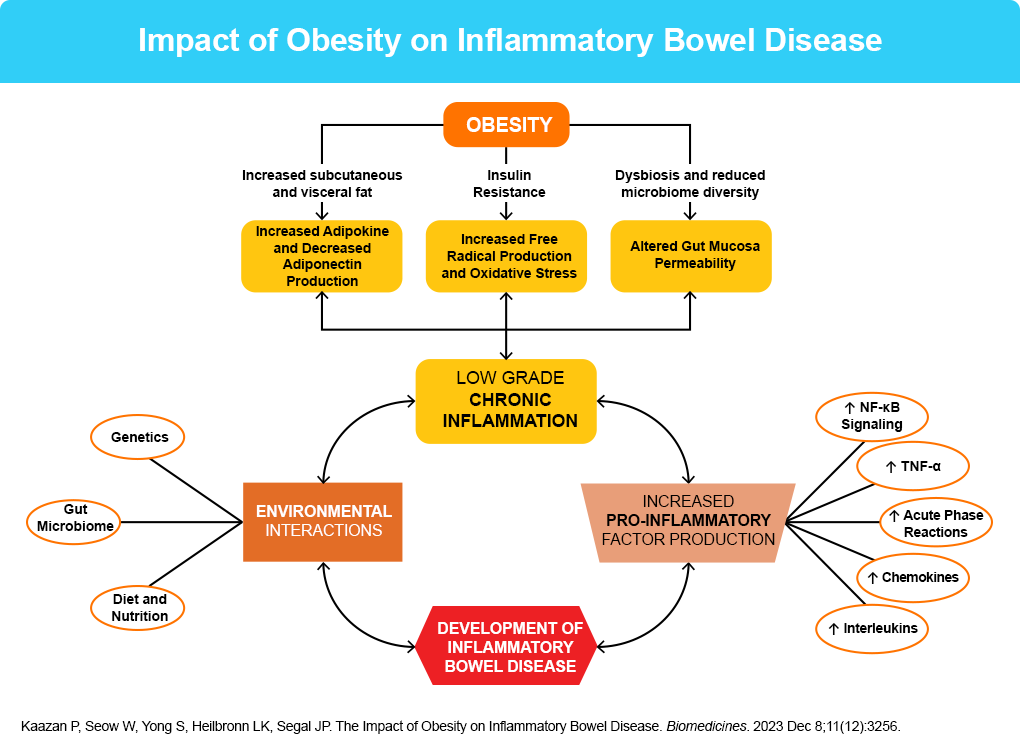
Patients with both obesity and Crohn’s disease exhibit a decreased diversity of microorganisms and characteristic changes in bacterial phyla, as well as evidence of abnormal gut bacterial translocation and inflammation.7,8 This translocation is an independent link to both obesity and Crohn’s disease. Central to IBD pathogenesis is mucosal barrier dysfunction, bacterial translocation, and loss of intestinal immune homeostasis.8 This has been linked to adipocyte and pre-adipocyte activation, with ensuing alterations in pro-inflammatory cytokine expression and immune homeostasis.5 Increased gut bacterial translocation is pertinent given its independent links to both obesity and Crohn’s disease; both conditions have a reduction in bacterial diversity with accompanying dysbiosis.7
Moreover, adipocytes stimulate activation of pro-inflammatory cells and produce mediators that increase systemic inflammation and influence mucosal homeostasis.9 Patients with IBD also show a unique locally restrictive form of visceral adipose tissue (VAT) — creeping fat — where mesenteric fat hyperplasia is limited to areas of inflamed bowel.10 Creeping fat is thought to be more immunologically active than other VAT, and the extent of creeping fat correlates closely with the extent of histological inflammation and degree of lymphocyte or macrophage infiltration.10
In addition to potential complementary pathologies, obesity might affect response to treatment for GI conditions, independent of drug exposure. For example, population pharmacokinetic studies of biologic agents approved for use in IBD, including infliximab, adalimumab, certolizumab pegol, golimumab, and vedolizumab, have identified high body weight as a risk factor associated with increased drug clearance, resulting in a short half-life and low trough drug concentrations.11
Ultimately, obesity and IBD – a potential proxy for other inflammatory GI conditions – create a vicious cycle involving intestinal barrier dysfunction and microbiota alteration, that, in turn, leads to the onset and maintenance of mucosal and systemic inflammation. Addressing obesity is thus essential for improving GI health. Dietary interventions and weight reduction, potentially with weight loss medications such as GLP-1/GIP receptor agonists, can alleviate microbiome dysfunction and also improve metabolic parameters, which can lead to resolution or improvement of obesity-associated GI conditions.
References
- Molodecky N, et al. Gastroenterology. 2012;142:46–54.
- Singh S, et al. Nat Rev Gastroenterol Hepatol. 2017;14:110–121.
- Singh S, et al. Gastroenterology. 2024;167:1307–1343.
- Zietek T, Rath E. Front Immunol. 2016;7:154.
- Karmaris K, et al. Inflamm Bowel Dis. 2006;12:100–105.
- Kaazan P, et al. Biomedicines. 2023;11:3256.
- Kim A. J Clin Gastroenterol. 2015;49(Suppl. 1):S20–S24.
- Dulai P, et al. Gastrointest Endosc. 2015;82:246–255.
- Pagnini C, et al. J Gastrointestin Liver Dis. 2024;33:542-551.
- Kredel LI, Siegmund B. Front Immunol. 2014;5:462-474.
- Bassi M, Singh S. BioDrugs. 2022;36:197-203.
